Sex: Female
Age: 26 years old
Urinary tract infections
The urinary tract is divided into:
Lower portion - urinary bladder and the urethra.
Upper portion - kidneys, renal pelves, and ureters
Upper urinary tract infections (UTIs) are most commonly ascending; they originate in the urinary bladder and ascend through the ureters to the kidneys.
The symptoms of upper UTIs are fever (often with chills) and flank pain. Frequency, urgency, and dysuria are more suggestive of infections of the urinary bladder and urethra (Lower urinary tract).
Community acquired UTI: Cystitis
Cystitis is caused bladder mucosal invasion, most often by enteric coliform bacteria (eg, Escherichia coli) that inhabit the periurethral vaginal introitus and ascend into the bladder via the urethra. Sexual intercourse may promote this migration, and cystitis is common in otherwise healthy young women.
http://www.emedicine.com/EMERG/topic626.htm
Community acquired UTI: Acute Pyelonephritis
Pyelonephritis is an ascending urinary tract infection that has reached the pyelum (pelvis) of the kidney. The causes are lower UTIs, mainly cystitis and prostatitis (but in this case, a woman does not have a prostate gland)
Williams DH, Schaeffer AJ (2004). "Current concepts in urinary tract infections". Minerva Urol Nefrol 56 (1): 15-31.
Discussion
The symptoms of upper and lower UTIs are relatively similar. Absence of catherter insertion inidcates that the UTI was not acquired in hospital. Thus the area of focus will be on community acquired UTIs. With consideration of the patient’s age and sex (26 years old female), it is highly probable that she is suffering from cystitis or acute pyelonephritis. In addition to the female urethra being shorter and nearer to the anus (anatomy), the fact that young women who are sexually active (26years old) will be more prone to cystitis (or communtiy acquired UTIs)
Small list of the common microbes related to UTI:
Escherichia coli – Common in young women, causes 80% of community-acquired UIT and 90% of the urinary tract infections (UTI) in anatomically-normal, unobstructed urinary tracts.
Staphylococcus saprophyticus - In young women, S. saprophyticus is, after Escherichia coli, the second-most-frequent causative agent of acute UTI
Proteus mirabilis - with functional or structural abnormalities or with long-term catheterization, forms bladder and kidney stones as a consequence of urease-mediated urea hydrolysis.
Pseudomonas aeruginosa - usually hospital-acquired and related to urinary tract catheterization, instrumentation or surgery
http://textbookofbacteriology.net/e.coli.html
http://iai.asm.org/cgi/content/abstract/72/5/2922
http://textbookofbacteriology.net/pseudomonas.html
Hovelius B, Mardh PA. (1984) “Staphylococcus saprophyticus as a common cause of urinary tract infections”. Rev Infect Dis. May-Jun; 6 (3): 328-37
Highly suspected microbes: Escherichia coli and Staphylococcus saprophyticus.
Tests
Dipstick tests
Dipstick tests are rapid and inexpensive, but need to be interpreted with caution. The two commonly used tests are the:
Leukocyte esterase test
Indicates pyuria by detecting esterases released from white blood cells. However, pyuria is not a specific indicator of infection.
Nitrate reduction test
Detects nitrites produced from nitrates by bacteria (mainly Gram-negative bacteria).
Dipstick tests are of most use as a negative screen

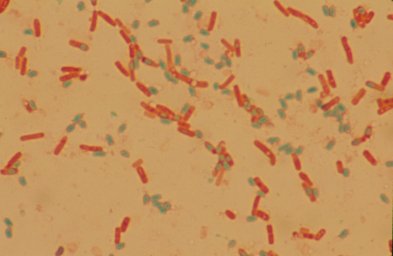
MacConkey Agar - mainly used in identification of lactose fermenting, Gram-negative enteric pathogens and for inhibiting growth of Gram-positive organisms. Bacterial colonies that can ferment lactose turn the medium red. This red color is due to the pH indicators response to the acidic environment created by fermenting lactose. Organisms that do not ferment lactose do not cause a color change.


Coagulase test - for differienting between pathogenic and non-pathogenic strains of Staphylococcus. A positive test is denoted by a clot formation in the test tube after the allotted time.

Indole test - When tryptophan is broken down, the presence of indole can be detected through the use of Kovacs' reagent. Kovac's reagent, which is yellow, reacts with indole and produces a red color on the surface of the test tube.

Oxidase test - If the bacteria oxidize the disk (remove electrons) the disk will turn purple, indicating a positive test. No color change indicates a negative test
http://medic.med.uth.tmc.edu >path >tests

Flow chart to direct the identification of serveral bacterial. (Main focus is on E. Coli)

A flow chart for the identification of Gram-Positive bacteria. (Staphylococcus saprophyticus not shown) Staphylococcus saprophyticus has the same characteristics as S. epdermidis, but Staphylococcus saprophyticus is resistant to novobiocin.
Use of Novobiocin-containing medium (sensitivity disks with 5 micro grams of novobiocin)
By demonstrating the resistance to the anti-microbial agent novobiocin, staphylococcus saprophyticus can be identified amongst the coagulase-negative staphylococcus.
http://web.indstate.edu/thcme/micro/staph/sld003.htm
Robert H. Latham, Grada A. Grootes-Reuvecamp, Dolores Zeleznik, and Walter E. Stamm. (1983). "Use of a Novobiocin-Containing Medium for Isolation of Staphylococcus saprophyticus from Urine." J Clin Microbiol. June; 17(6): 1161–1162.
-Willie-