Patient 4: Ng Ming En
Diagnosis: Food Poisoning
Complaints: Severe vomiting, diarrhea, abdominal cramps
Findings:
Foodborne illness (food poisoning) results from eating food contaminated with bacteria (or their toxins) or other pathogens such as parasites or viruses.
After they are swallowed, there is a delay, called the incubation period, before the symptoms of illness begin. This delay may range from hours to days, depending on the organism, and on how many of them were swallowed. During the incubation period, the microbes pass through the stomach into the intestine, attach to the cells lining the intestinal walls, and begin to multiply there. Some types of microbes stay in the intestine, some produce a toxin that is absorbed into the bloodstream, and some can directly invade the deeper body tissues. The symptoms produced depend greatly on the type of microbe. Numerous organisms cause similar symptoms, especially diarrhea, abdominal cramps, and nausea.
Diagnosis: Food Poisoning
Complaints: Severe vomiting, diarrhea, abdominal cramps
Findings:
Foodborne illness (food poisoning) results from eating food contaminated with bacteria (or their toxins) or other pathogens such as parasites or viruses.
After they are swallowed, there is a delay, called the incubation period, before the symptoms of illness begin. This delay may range from hours to days, depending on the organism, and on how many of them were swallowed. During the incubation period, the microbes pass through the stomach into the intestine, attach to the cells lining the intestinal walls, and begin to multiply there. Some types of microbes stay in the intestine, some produce a toxin that is absorbed into the bloodstream, and some can directly invade the deeper body tissues. The symptoms produced depend greatly on the type of microbe. Numerous organisms cause similar symptoms, especially diarrhea, abdominal cramps, and nausea.
Culture
To find out what is the organism, the specimen (stools) is send for culturing using agar plates.
Inoculated places are O2 incubated unless otherwise indicated.
All faeces are inoculated onto the following media: BAP, MAC, SS, Selenite broth and Campylobacter selective agar for the isolation of salmonella, Shigella and Campylobacter spp.
In addition to the above:
· Bloody faeces are also inoculated onto Sorbitol MAC plate.
· Watery faeces are plated on TCBS and inoculated onto APW to culture for Vibrio spp.
Common Bacteria found in Bacterial gastroenteritis

Inoculated places are O2 incubated unless otherwise indicated.
All faeces are inoculated onto the following media: BAP, MAC, SS, Selenite broth and Campylobacter selective agar for the isolation of salmonella, Shigella and Campylobacter spp.
In addition to the above:
· Bloody faeces are also inoculated onto Sorbitol MAC plate.
· Watery faeces are plated on TCBS and inoculated onto APW to culture for Vibrio spp.
Common Bacteria found in Bacterial gastroenteritis

Then gram staining is performed to determine whether organism is gram positive or negative. Following that, the organism shape (cocci or bacilli) is also determined and biochemical test is determined.the biochemical testsare used to detect the presence of enzymes (eg. Catalase, oxidase etc) and metabolic end-products (eg. Methyl red, etc). Lastly, an antibiotic sensitivity test is performed.
The above steps are performed to determine the organism and the organism I suspected is:Bacillus cereus
Some info about Bacillus Cereus
Bacillus Cereus food poisoning is a gastrointestinal intoxication caused by toxins produced by the Bacillus Cereus bacteria. It is a gram-positive spore-forming organism found in soil and dust. It is frequently found in rice dishes, occasionally pasta, meat or vegetable dishes, dairy products, soups, sauces and sweet pastry products where these have not been cooled quickly and effectively after cooking and during storage. It causes two different forms of food poisoning: an emetic illness and a diarrhoeal illness. The emetic illness ismediated by a highly stable toxin that survives high temperatures and exposure to trypsin, pepsin and pH extremes. The diarrhoeal illness is mediated by a heat- and acid-labile enterotoxin.
B. cereus-associated foodborne illness occurs as 2 distinct syndromes: emetic and diarrhoeal.
Incubation: Emetic; 1-6 hours after eating contaminated food.
Diarrhoeal; 10-12 hours.
Symptoms: The symptoms of the emetic syndrome result from ingestion of pre-formed toxin: nausea and vomiting, occasionally followed by diarrhoea. Diarrhoeal symptoms results from ingestion of vegetative organisms or spores and their subsequent multiplication and toxin production within the intestinal tract: abdominal pain, watery diarrhoea and occasional nausea

The above steps are performed to determine the organism and the organism I suspected is:Bacillus cereus
Some info about Bacillus Cereus
Bacillus Cereus food poisoning is a gastrointestinal intoxication caused by toxins produced by the Bacillus Cereus bacteria. It is a gram-positive spore-forming organism found in soil and dust. It is frequently found in rice dishes, occasionally pasta, meat or vegetable dishes, dairy products, soups, sauces and sweet pastry products where these have not been cooled quickly and effectively after cooking and during storage. It causes two different forms of food poisoning: an emetic illness and a diarrhoeal illness. The emetic illness ismediated by a highly stable toxin that survives high temperatures and exposure to trypsin, pepsin and pH extremes. The diarrhoeal illness is mediated by a heat- and acid-labile enterotoxin.
B. cereus-associated foodborne illness occurs as 2 distinct syndromes: emetic and diarrhoeal.
Incubation: Emetic; 1-6 hours after eating contaminated food.
Diarrhoeal; 10-12 hours.
Symptoms: The symptoms of the emetic syndrome result from ingestion of pre-formed toxin: nausea and vomiting, occasionally followed by diarrhoea. Diarrhoeal symptoms results from ingestion of vegetative organisms or spores and their subsequent multiplication and toxin production within the intestinal tract: abdominal pain, watery diarrhoea and occasional nausea
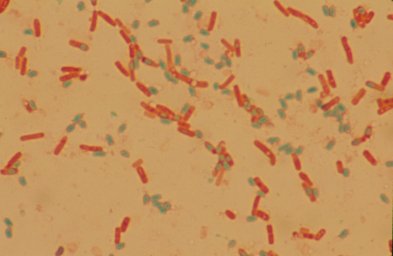
a picture of bacillus cereus
Adapted from: http://textbookofbacteriology.net/B.cereus.html
Another organism that i suspect in this patient is: Vibrio cholerae
References
http://www.foodlink.org.uk/factfile_c.asp?file=1&chapter=9
http://www.cdc.gov/ncidod/dbmd/diseaseinfo/foodborneinfections_g.htm
http://www.nzfsa.govt.nz/science/data-sheets/bacillus-cereus.pdf
http://www.foodlink.org.uk/factfile_c.asp?file=1&chapter=9
http://www.cdc.gov/ncidod/dbmd/diseaseinfo/foodborneinfections_g.htm
http://www.nzfsa.govt.nz/science/data-sheets/bacillus-cereus.pdf
posted by Huiling